



The Devizes to Westminster Canoe Marathon
A little over 35 hours is how long it took David Burton and Mattie Morgan to paddle 125 miles from Devizes in Wiltshire to Westminster in central London - a hugely demanding and impressive feat. We are incredibly grateful for their dedication to the Foundation. David shares their story below:

The Race
Amazingly, almost unbelievably…I am absolutely delighted to report that Mattie and I made it to Westminster!
We are incredibly pleased, proud
and relieved all rolled in one. It’s
still sinking in.
114th out of 145 starters, with
31 retirees.
The world’s longest non-stop
canoe race – 125 miles, 77 locks, paddled non stop. It is billed as one of the toughest endurance
events of its kind. I had quite
forgotten that bit… It requires close
teamwork between both the crew and the support group, and huge amounts of
empathy, understanding and determination.
Without it you won’t succeed.
We hit all the cut off times down
the course this time, but were slowed down by the conditions and just missed
the second tide window at Teddington on Easter Day. Which meant we had to wait until 0610 on the
Monday to set off again on the next tide, arriving at Westminster Bridge at
0900.
Conditions were pretty tough –
really hot during the day and really cold at night, thick mist and fog, no flow
on the Thames and really rough water just before Westminster. Many paddlers pulled out or were pulled out
of the race for a host of reasons. And
incredibly sadly, as you may have read in the press, one paddler died shortly
after reaching the finish.
Our time was officially circa 44:24:57…. But it was actually circa 35 hours paddling for us without the short Teddington stop-over (which put us ahead of some of the other non-stop finishers!).
The Finish and the Team
This was an amazing experience
overall on so many levels - pretty emotional at the finish; a mere 34 years
after my first finish with my very good friend Robert Martine who was there at
the finish this time too.
We could not have done it without
our amazing and ever patient support group.
Or without Simon Jones (who
amongst other things is in charge of kayaking at Bryanston School and has been
incredibly supportive of us throughout) whose amazing no-nonsense and positive
attitude towards the end helped push us to hit the final cut off time.
Or without the friends and family
who kept sending messages throughout and who also popped up from time to time
along the course – even if sometimes we didn’t actually see or hear them
because we were so tired!
And I certainly could not have done it without my very long suffering, but still very good friend, Mattie Morgan, who’s own determination and positive "can do" attitude helped pull me through on many occasions.



STAE Course April 2019
One of the key missions of this foundation is to provide specialist training to doctors and surgeons who would otherwise be unable to afford it. Our STAE courses help to meet this aim. These courses equip surgeons with specialist skills in how to work in conflict and disaster zones. Your support enables us to offer scholarships to surgeons who work in these challenging conditions. It costs £5,000 per student and we cover this entire cost through your generosity. On this course, delivered at the start of April 2019, training covered how to care for eye injuries from blast wounds, as well as a number of other elements of specialist surgery.
This course was attended by 13 surgeons from around the world including Nepal, Syria, Uganda and Chile. These are some of their stories
Introducing Lucien

Lucien Wasingya Lusenge is a general surgeon in Uganda and works in a rural area 100km from Kampala. He told us that healthcare in Kampala is expensive and not available to most people in rural areas of Uganda.
Lucien regularly sees patients with severe injuries from
road traffic accidents. He's been telling us that many of these patients die
unnecessarily because they're not properly managed due to lack of resources and
specialist skills.
Because of the STAE course, Lucien feels more confident that these patients will now have better outcomes and many more lives will be saved "Thank you for the training. I am so proud to be among the trainees".
Introducing Tula and Pawan

Tula Gupta and Pawan Bajaj Agrawal joined us from Nepal. They are both GPs and work in a rural area of the country where there are no surgeons. Being some distance from Kathmandu and the only medics in the area, they have to do everything including surgery such as orthopaedics, caesarians and trauma.
They work in a natural disaster area where there are lots of small earthquakes. Tula told us "Since the 2015 earthquake, we have been re-building the health system in Nepal. The course has been a great opportunity to learn so many things and supplement my knowledge to do even more difficult cases."
Introducing Awss

Awss Alhamadani is a surgeon working in Iraq. He had previously been on our overseas training course and came to the UK as one of our scholars to gain additional practical training. Responsible for eight field hospitals in Iraq, Awss is able to share his additional skills and expertise with his colleagues who often work with limited resources and in very challenging conditions. Aware of the impact these courses have on the provision of treatment in the hospitals under his care, Awss wrote to the both the Prime Minister and Minister of Health in Iraq recommending "that, every single person who enters into surgery, should have this course."
The scholars tell us that the way the course is organised is invaluable. "We're taught the procedure first as a whole group and then get to practice it afterwards in a small team under the supervision team of a surgeon from the Faculty Team," all of whom are expert surgeons with first hand experience of working in a conflict zone.
We heard from Vadvm who joined us from Ukraine; "This course is way beyond my expectations. It is the best thing that has happened to me in the field of austere environment surgery."
We're delighted to share these stories, and hear how our course will bring about better health outcomes for patients and save lives. Every one of our scholars works in very challenging conditions, whether it's with limited resources, personnel or in an austere environment like a conflict zone or area affected by natural disaster.
We're proud to be fully funding our scholars on the course. Through your generosity their travel, accommodation and course fees are all covered. Without your support, none of this would be possible.

Mission to Lebanon
In early March 2019, we ran a surgical mission to Lebanon with Syria Relief to support Syrian and Palestinian refugees living in refugee camps. The work done by the teams involved everything from repair of blast injuries from conflict to skin grafts for burns, as well as more routine operations.
With your support we were also able to run primary care
clinics for day-to-day healthcare issues. David also taught surgical procedures
to local surgeons in Lebanon giving them the specialist skills needed to work
with victims of conflict.
We've been hearing from one of the doctors on the mission, who told us: "This work not only invests in the local surgical team, but also provides life changing operations free of charge for Syrian and Palestinian refugees who would not be able to access this treatment otherwise."

Yemen HEST® January 2019
The David Nott Foundation ran two HEST® courses in Aden, Yemen in January 2019 with the support of Médecins Sans Frontières.


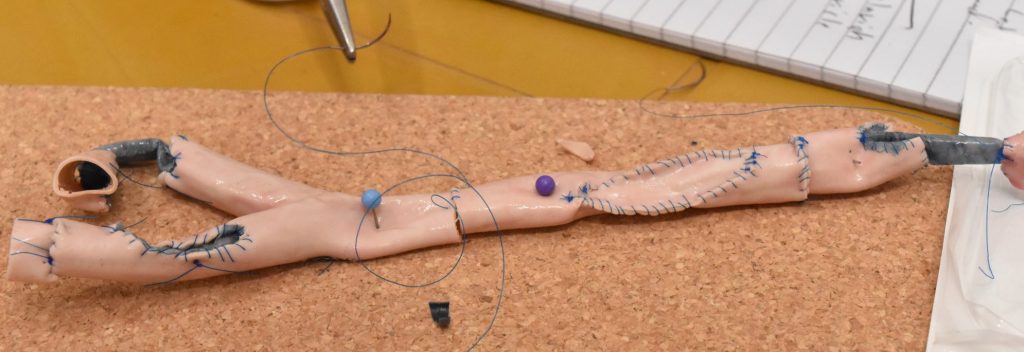
These two HEST® courses were the first occasion that the Foundation’s whole body simulator was employed for training and supporting it was a suite of individual models of organs, blood vessels and key anatomies with which the students could train. For the obstetrics modules, the Faculty used its commercially-sourced obstetrics simulator enabling each surgeon to practise multiple Caesarean section deliveries as well as neonatal resuscitation.
Training
Covering 2-5 hours each, the courses were taken through:
- Ballistics – the effects of low velocity bullets and high velocity bullets and the four stages of a blast injury on the human body
- Primary and secondary survey
- Damage control
- Cardio-thoracic trauma – thoracotomies; lung twist and tractotomy; effects of a cardiac tamponade; pericardial sac opening; heart suturing
- Vascular surgery – ligating, shunting, patching and grafting vessels; fasciotomies; proximal and distal control
- Head and neck trauma – removal of extracranial haematoma; burr holes and craniotomies for extradural haematoma; fragment removal with depressed skull fractures; treatment of mandibular and Le Fort fractures; jaw and maxilla wiring
- Principles of paediatric surgery – differences in physiology; burns; common injuries and diseases; cultural considerations
- Abdominal trauma – laparotomies; control of bleeding; pelvic injuries and bracing; splenectomy; Cattel-Braasch manoeuvre; Whipple procedure; bowel anastomoses; ileostomy and colostomy; closure of abdomen
- Orthopaedic surgery – stabilisation by plaster of Paris; traction; external fixation; management of difficult fracture, non-union and infection; osteomyelitis; amputations
- Plastic surgery – burns; debridement and reconstruction; skin grafts; tissue flaps
- Trauma in obstetrics and gynaecology – vaginal deliveries; Caesarean sections; hysterectomies; post-partum haemorrhage with compression techniques and tamponade; perineal trauma; retained products; ectopic pregnancy; neonatal resuscitation



Students
The Faculty trained 52 students over the two courses. 20 surgeons and doctors from across the country came for the first week and demonstrated a high level of experience and skill, and engaged well with all the training, even putting some of it into use the same day once they returned to theatre. By the time the second course started the work had spread and many more than expected turned up to start, with some having to be turned away to keep the numbers manageable.
Particularly interesting was the attendance of five surgeons who had previously attended a HEST® course delivered by David and team in Aden in 2016. Among those was a highly respected female surgeon; the only in Aden and possibly the only in Yemen, who had only recently qualified. In the three years since she had come to be regarded as a one of the best there and consistently impressed the Faculty. Such was her appetite to learn that she even sat in on some of the sessions in the second week to make sure it was all sinking in.
Conclusion
There is no doubt in our minds as to the value of the courses in Yemen and the evidence of and potential for making a very real difference to the surgical outcomes for patients not only treated by the surgeons we taught, but also those to whom the training, techniques and procedures can be cascaded.
The impact that the models have made is exceptional; they have transformed the course and are now invaluable training aids for almost all components of the syllabus. Both the surgeons that have trained with the models, and the David Nott Foundation faculty that have used it in their teaching, have been emphatically enthusiastic in their feedback about the value it brings to the training. Both the surgeons that have trained with the models, and the David Nott Foundation faculty that have used it in their teaching, have been emphatically enthusiastic in their feedback about the value it brings to the training.




HEST® in Libya
It was the early hours of 4 March when our DNF team touched down at Misrata airport. David and Ammar were this time joined by Harald Veen, formerly Chief Surgeon of the Red Cross and now a valued addition to our teaching faculty.
Over the next three days they taught 55 Libyan doctors in the skills they need to provide the best surgical care for patients with complex injuries.
The doctors had travelled from across the country from towns including Tripoli, Misrata, Houn and Sabha. The majority specialised in general surgery but there were also orthopaedic surgeons, an obstetrician and a neurosurgeon present; demonstrating the relevance of our training programme to all medical specialities.
 HEST® faculty in Misrata
HEST® faculty in Misrata

The course concluded with a practical workshop at Misrata Central Hospital where they put their newly-learnt skills into practice with tuition from David, Ammar and Harald on vascular, general surgical, neurosurgical and facio-maxillary techniques.

We have already had three applications for scholarships from surgeons attending the Misrata course and look forward to continuing to build our friendships with the doctors of Libya.





Yemen HEST® July 2016
David Nott Foundation ran a HEST® course in Aden, Yemen from 10-12 July, 2016. 43 surgeons from hospitals in Aden, Lahj, Abyan, Lawder and Shabwa attended the three-day war surgery training.
David showed the doctors how to treat a variety of complicated war injuries, principally fragmentation and gunshot wounds. There had been an increase in suicide bomb attacks and bombs placed under cars in recent weeks, causing horrendous blast injuries which David also showed the doctors how to treat.
The Foundation taught the course at the invitation of Médecins Sans Frontières (MSF) as part of their regular training for local doctors and nurses.
David said: “I was thrilled to receive the invitation from MSF to run the HEST® course in Yemen and am delighted to say we have had more invitations to run courses from other aid agencies in various countries. It shows the huge importance of the work we are doing and the very real need for surgical training in war zones.”





The BMJ: Training Idlib’s obstetricians
Giving birth is one of the most vulnerable moments a woman can experience. It can be anxiety-inducing enough in a well-equipped hospital in the UK, but the women of Idlib, Syria are literally having their babies in a warzone. The threats they face are myriad, not only to themselves and their babies, but also to the physical fabric of the hospital and the medical workers who care for them. In early September the Has hospital was barrel-bombed and put out of action. Ambulance stations and a Syria Civil Defence (White Helmets) first response centre were also put out of service.
Beneath the headlines about “shapeshifting” rebel groups which have formed, fractured, and re-formed over the course of the civil war, and deals cut in regional capitals, is the suffering of the civilian population of Idlib, the last province in Syria not under regime control.
The numbers are stark; 336 maternal deaths per 100,000 births in provinces outside government control in Syria. [1] There are 9 per 100,000 in the UK. The figures for neonatal deaths are similarly distressing; 30.6 deaths per 1,000 births in Idlib compared to 3/1,000 in the UK. [2]
Violence against hospitals and medical staff affects clinical decision-making.
On 19 March 2018, the Union of Medical Care and Relief Organisations (UOSSM) reported that doctors in eastern Ghouta had, on the previous day, performed 15 caesarean sections out of a total of 30 births. The doctors said that they were being forced to do caesareans as the intense besiegement made it difficult for expecting mothers to predict when they could safely go to the hospital. The risk of complications for the mother and child are increased by the lack of incubators, medical equipment, and staff with the right training to perform follow up care.
However, the war alone cannot explain the high levels of maternal and neonatal morbidity. There is a serious shortage of obstetricians and midwives to care for a population of some 3 million. This can lead to non-specialists having to undertake the care of pregnant women and neonates and sometimes not making the correct decision for the patient. While not all of that population of 3 million will be having children, of course, the pressure on health services has increased as much of that population is made up of internally displaced people from areas including eastern Aleppo, eastern Ghouta and Homs. The province has become a receptacle for the vanquished as the regime has hammered those opposed to Assad’s rule. Following relentless campaigns of bombing and the use of chemical weapons, those civilians left alive boarded buses for Idlib province.
Among those on the green buses heading for Idlib in December 2016 was Farida; known as the last obstetrician in eastern Aleppo. Farida made impassioned pleas for the indiscriminate bombardment of her City to stop on several media channels in 2016. Her departure with her husband and daughter is an evident source of present pain, but there was something about those months leading up to the evacuation. “We made a difference. We were working so hard and helping so many people. Though we were under constant attack, we were part of something extraordinary and saving lives every day.”
Farida and 17 other obstetricians were in Gaziantep recently for Systematic Management and Emergency Care in Obstetrics and Midwifery (SMEC-OM), a course organised and funded by the David Nott Foundation, Hand in Hand for Aid and Development, and World Vision International. The Syrian civil war has stalled the medical education of doctors and midwives, a further major contributing factor to the poor outcomes in obstetrics and gynaecology. Postpartum haemorrhage and eclampsia/pre-eclampsia were responsible for the majority of maternal deaths in areas of Syria not under government control in 2017. [3] The SMEC-OM has been devised to save the lives of mothers and babies by training clinicians to use established algorithms and guidelines for managing conditions such as maternal collapse, post-partum haemorrhage, pre-eclampsia, sepsis, and neonate resuscitation. The Royal College of Obstetricians and Gynaecologists (RCOG) in London is supporting these efforts and the course is conducted under the auspices of its Syrian Liaison Group.
Organising this essential training is Saladin Sawan, a British-Syrian gynaecologist. Saladin is joined by a faculty of trainers from several Arab states, all of whom give up their time for free. They lecture with authority and passion for their subject, inviting debate and questions from the doctors, 90% of whom are women. The energy in the room is palpable as they question graphs and diagrams and participate in practical exercises on specialist obstetric simulator models.
What they learn is being measured by an exam comprising both a paper of multiple-choice questions and a practical assessment on a simulator. The candidates who perform most strongly in the assessment proceed to a “train the trainers” day, where they will be coached to provide help and supervision to their colleagues in Idlib. This is especially important as 35 candidates had registered to attend the training but only 18 were able to make it across the Turkish border.
Getting the best in surgical training to those who need it most is the mission of the David Nott Foundation and we were proud to be able to support this thorough, detailed training.
In the coffee area I meet Abdulaziz. Before the war, Abdulaziz was a surgeon at Aleppo University Hospital and lecturer at the University’s faculty of medicine. With a small group of others, he was instrumental in locating safe houses where emergency operations could be performed on wounded protesters in the early days of the revolution. At night he gave lectures to medical students over Skype; focusing on emergency first aid and treating gunshot wounds. [4]
It is the focused effort of Abdulaziz, Saladin, and countless other individuals and charities that has created a shadow health system in areas of Syria not under government control. As the Syrian regime and its Russian supporters bombed hospitals and medical facilities, they scrambled to set up new ones underground and in caves. As the number of doctors shrank, they strove to train and upskill those who remained.
Idlib is the final front in the Syrian civil war and it is uncertain whether the current ceasefire will hold. The diplomats and politicians negotiating Syria’s fate owe it to the obstetricians I met in Gaziantep, and the thousands of women and babies who depend on them, to come up with a solution which creates the peace, security and dignity they so greatly deserve.
Elly Nott, Co-Founder and Chief Executive, David Nott Foundation
References:
1] 2017 survey conducted by the Syrian Board of Medical Specialities (SBOMS), “article in preparation”
2] World Bank data
3] 2017 survey conducted by the Syrian Board of Medical Specialities (SBOMS), “article in preparation”
4] Ben Taub, ‘The Shadow Doctors,’ The New Yorker, June 27, 2016 Issue
Originally posted on: https://blogs.bmj.com/bmj/2018/11/09/elly-nott-training-idlibs-obstetricians/

The Mail on Sunday: My secret mission to save Aleppo’s babies of the blitz
David Nott writes for The Mail on Sunday
Of all the wounded children of Aleppo who passed before me, the memory of one has lodged in my mind like no other. Maram. I spent the week before Christmas in a field hospital in Syria operating on many tiny souls see-sawing between life and death, their bodies held together with metal pins and scaffold-like fixators.
But in Maram, a five-month-old orphan and beautiful despite her injuries, I saw my own child and, perhaps because I missed her so desperately, I felt intensely overwhelmed.
I have made numerous trips to Syria to treat the casualties of this war, but none was as sorrowful as the week I spent with Aleppo’s children. Bone-weary and drained emotionally, I returned to London on Christmas Eve and couldn’t wait to hold my 17-month-old daughter and see my wife and family. Christmas was a joy.
Yet Maram was never far from my mind’s eye: a haunting, residual memory that I could not have shaken even if I had wished; I find myself waking in the early hours worrying about her. I first saw Maram on December 20, a few days after she was evacuated from Aleppo in an ambulance. Her legs and left arm had been shattered in a bomb attack that killed her parents and injured her brother and sister.
Pieces of ordnance shell were embedded in her infected wounds but, because the Aleppo doctors had run out of dressings, disinfectant and saline, they had no choice but to operate on her dirty body tissue. As I looked down at Maram on the treatment table she was crying, not because she was tired and hungry, even though she was both, but because she was in great pain.
There are no paediatricians in Aleppo, or at the hospital where I was working; nobody qualified to make the very difficult decisions about how much analgesics and fluids to dispense. So in spite of all her suffering, Maram was simply on a small dose of paracetamol. It was heartbreaking. I checked her charts. In the UK, these would have been filled in with scrupulous attention to detail, but in Syria, with doctors battling to save the lives of so many, charts were overlooked. I couldn’t even tell what medication she had already received.
Maram wriggled uncomfortably. I tried to think logically about how to help her and what I’d need to do when I operated on her the following day. But precise thought was difficult as I felt myself experiencing the same sort of emotions that any father would have towards a wounded child.
I operated on December 21, carefully debriding Maram’s wounds and removing the decaying tissue inside her. The whole hospital stank of the bacteria that had caused her infections, and those in other patients. I worked delicately around the open compound fracture Maram had suffered in her left leg.
Correctly in my opinion, the surgeon who had operated on her in Aleppo had applied an external fixator, but this was so big and heavy that Maram couldn’t move her leg when she was awake. It was so sad to see. She also had a pin in her femur and another in her tibia, and she had a really big gap of leg bone missing from the explosion.
Read more here.
The Observer: In Aleppo’s destroyed hospitals the dead lie with the living
David writes for The Observer
I don’t think that in all my years of doing this I’ve ever seen such dreadful pictures of injuries, of people lying on the floor of an emergency room, the dead mixed with the living.
One colleague, who I speak to all the time, was in despair, sending me all these photographs, and saying: “David, you have to do something to help us.” But what can I do?
The message out of eastern Aleppo is that there are no hospitals functioning at all. They have all been repeatedly attacked in the past few days. Some were able to evacuate, but one was totally and utterly destroyed by rockets and bombs. I heard that two doctors were killed and 16 other staff injured and I am afraid that one of the dead may be a brilliant surgeon, who would be a particularly serious loss.
There is another hospital that we haven’t even had a message from. So, I suspect they are out of action, but we know nothing about the staff or the conditions there.
The Aleppo hospitals have been re-opened so many times, underground or at new locations, but between the bombing and the siege I don’t know if it will be possible to resurrect them this time. There is so much equipment that you need in order to operate and there is no sterilisation and no monitoring machines for anaesthetics. Even if the hospitals saved some machines they can’t run them because the generators have been destroyed or are out of fuel.
The taking out of every hospital and medical facility that gives hope and help to civilians is not a coincidence. The medics have such fantastic morale that you would not imagine them giving up, but I have an awful suspicion that this is the endgame.
Read the full article here.