



Four Years of the David Nott Foundation
Today we are celebrating four years of the David Nott Foundation.
Thank you for your support; for four years of running marathons, training surgeons, technological pioneering and building global networks.
Throughout the week on social media we have been highlighting some of the achievements that we have made so far:
We have taken our Hostile Environment Surgical Training (HEST®) course to nine countries, running twelve courses with seven partner organisations. The result of this has been that 543 doctors have now been trained in cutting-edge surgical techniques that, in conflict and disaster zones, will mean the difference between life or death.
Back in the UK, we have collaborated with the Royal College of Surgeons of England to produce six Surgical Training for Austere Environments (STAE) courses, bringing surgeons and doctors from 25 countries to London to complete this unique course. We are particularly proud that we were able to offer 62 full scholarships for these courses, widening our outreach and reducing barriers to accessing this life-changing training for surgeons who would not otherwise be able to participate.
Our global family of physicians, surgeons, doctors, donors and supporters is growing every day. The stories we hear from all involved are both humbling and inspiring. We look forward to the next four years with excitement and determination, and hope you will join us in our endeavour.
Conflict doesn't stop, and neither do we: we have helped to save 1.3 million lives and limbs but can help so many more. Find out how you can get involved and donate to the Foundation on our 'Get Involved' page, or suggest any fundraising ideas in an email to [email protected].

Newsletter July 2019
This is our latest news update from the David Nott Foundation. In this month's issue:
- The David Nott Foundation turns four years old!
- Introducing Heston®: our silicon cadaver transforming surgical training
- We highlight one of our #wardoctorheroes, Dr Omar from Iraq

This week we celebrate four years of the David Nott Foundation. Thanks to your support, we have been able to achieve such a huge amount in this short time.
We have taken our Hostile Environment Surgical Training (HEST®) course to nine different countries, running 12 courses with seven partner organisations; there are more on the way and word is spreading fast. Through lectures and simulations, HEST® has improved complex surgical skills and built a global network of war doctors, equipped to deal with the most hostile of surgical environments. Read more about HEST®...
On the other side of our work, we have brought surgeons from 25 countries to six UK-based Surgical Training for Austere Environments (STAE) courses, run by the Royal College of Surgeons. The Foundation has been able to award 62 scholarships to surgeons who otherwise would not have been able to carry out the training.
Read more about STAE...
What drives our world-leading status in surgical training is a combination of pioneering innovative technologies, highly effective methods of teaching, and an exceptional team devoted to bridging the gap between the Foundation's faculty and the surgeons who can benefit from them.
Conflict doesn't stop, and neither do we. Your support has helped us achieve so much already but there is more to do. Head to our website to find out how you can get involved, fundraise or donate to ensure that we can continue to train surgeons, and save lives.
Introducing Heston®: the silicon cadaver saving lives

When training surgeons to perform complex procedures in hostile war zones, or natural disaster areas, it can be very difficult to simulate operations on the go; cadaver training that would be used in the UK has been impossible on our HEST® courses.
Enter Heston®: a full-sized and incredibly accurate silicon patient named after our HEST® programme. Created by Max and Izzy Campbell, Heston® is fully equipped with all the incisions and realistic internal organs necessary to demonstrate the trauma surgeries that save people's lives in hostile environments. Heston® has already travelled with us to Yemen and Kenya, and as a dedicated honorary faculty member, he will continue to help us in future locations.
Heston® is the latest example of the David Nott Foundation's technological innovation. Advancements in surgical teaching equipment such as Heston® mean that our war doctors are better prepared to face real casualties with advanced techniques.
Let Heston's® creators introduce him further in this video.
Spotlight on Dr Omar Alamouri
The Foundation's global network of #wardoctorheroes is our proudest achievement. Our work is about investing in people, providing the skills that save lives.
Hailing from Iraq, Omar is an orthopaedic surgeon who came to one of our surgical training courses in 2018. He was awarded a David Nott Foundation scholarship, which allowed him to travel to the Royal College of Surgeons in London to attend the Surgical Training for Austere Environments (STAE) course directed by David Nott.
Following Omar's completion of the STAE course, and now home in Iraq, a massive road traffic accident saw a young patient brought into hospital. With a compound hip fracture, and rapid blood loss, doctors were gravely concerned that he would not survive.
With a rapid and calculated reaction, Omar performed a life-saving procedure that he had learned on our training course. He hoped to give his young patient the greatest chance of survival.
We are pleased to say that he recently visited his patient, who is now doing well. Speaking about the Foundation he said:
"You saved another life without even knowing [it]. You all should be proud of what you are doing. I want people to know the real benefits of these training courses”.


War Doctor Heroes: Meet Dr Omar
This is Omar. He is an orthopaedic surgeon in Iraq. He came on one of our surgical training courses in 2018.
We heard that, following a massive road traffic accident, a young patient was brought into his hospital with a compound hip fracture. He was losing so much blood that doctors were gravely concerned that he might not survive. Omar decided to perform a procedure he'd learnt to do properly on our training course.
He recently visited his patient and was delighted to see that he's doing really well. "You saved another life without even knowing it. We are so proud of you. I want people to know the real benefits of these training courses".
"The training helped me to do the procedure properly and without it the boy may not have lived" said Omar.
Help us train more surgeons like Omar https://lght.ly/1jbkc1g

Meet Heston®!
Our newest team member is Heston®: a life-sized replica human crafted from silicon. Heston® plays a leading role in our overseas training programmes, so far helping us in Yemen and Kenya.
Named after our Hostile Environment Surgical Training (HEST®) course, Heston’s® intensive design and ingenious construction process ensure that his skin, bones and organs feel and look authentic. This anatomical accuracy provides surgeons with a close-up look at what they can expect during real field operations, and difficult procedures in austere environments.
Thanks to Heston’s® creators Max and Izzy Campbell (@healthcuts on Instagram); their work keeps us at the cutting edge of technologies that will train war doctors, and save lives.

Taking on the Great North Run
Frederick Watson is running the Great North Run for the David Nott Foundation!
Frederick grew up in Newcastle and did the Great North Run for the first time in 2002. He now lives in South Island, New Zealand, and will be strapping on his running shoes and flying back this year to run again.
He was inspired by War Doctor, which he found in his local library, and he has even recommended it to his son to read too. The pair will be running together in September. If you want to show your support for Frederick, you can find his fundraising page here: https://www.justgiving.com/fundraising/frederick-watson1
Thank you Frederick!
Newsletter May 2019

Welcome to our latest news and round-up of how your support has been helping us to train more doctors with the specialist medical skills they need to work in war and disaster zones.
David Nott in conversation with Sarah Montague 
On the evening of the 30th April, David was joined in conversation with the BBC’s Sarah Montague at the Saatchi Gallery to discuss his book, War Doctor. He shared stories of his work around the world in war zones and why he and Elly set up the Foundation to share his knowledge and expertise with local doctors working on the ground. Sarah asked him how many lives he thinks he’s saved through his own work overseas in war zones and also through our training programme “Possibly in the hundreds of thousands,” David replied.
Among the guests was actor and former doctor (of another variety) Peter Capaldi. He noted that the evening was “a humbling and inspiring experience, meeting both David and Elly.”
We are delighted to report that, through the generosity of all those who attended the event, enough money was raised to provide equipment to train more than forty surgeons as well as award ten fully-funded scholarships to surgeons currently operating in war zones and disaster areas.
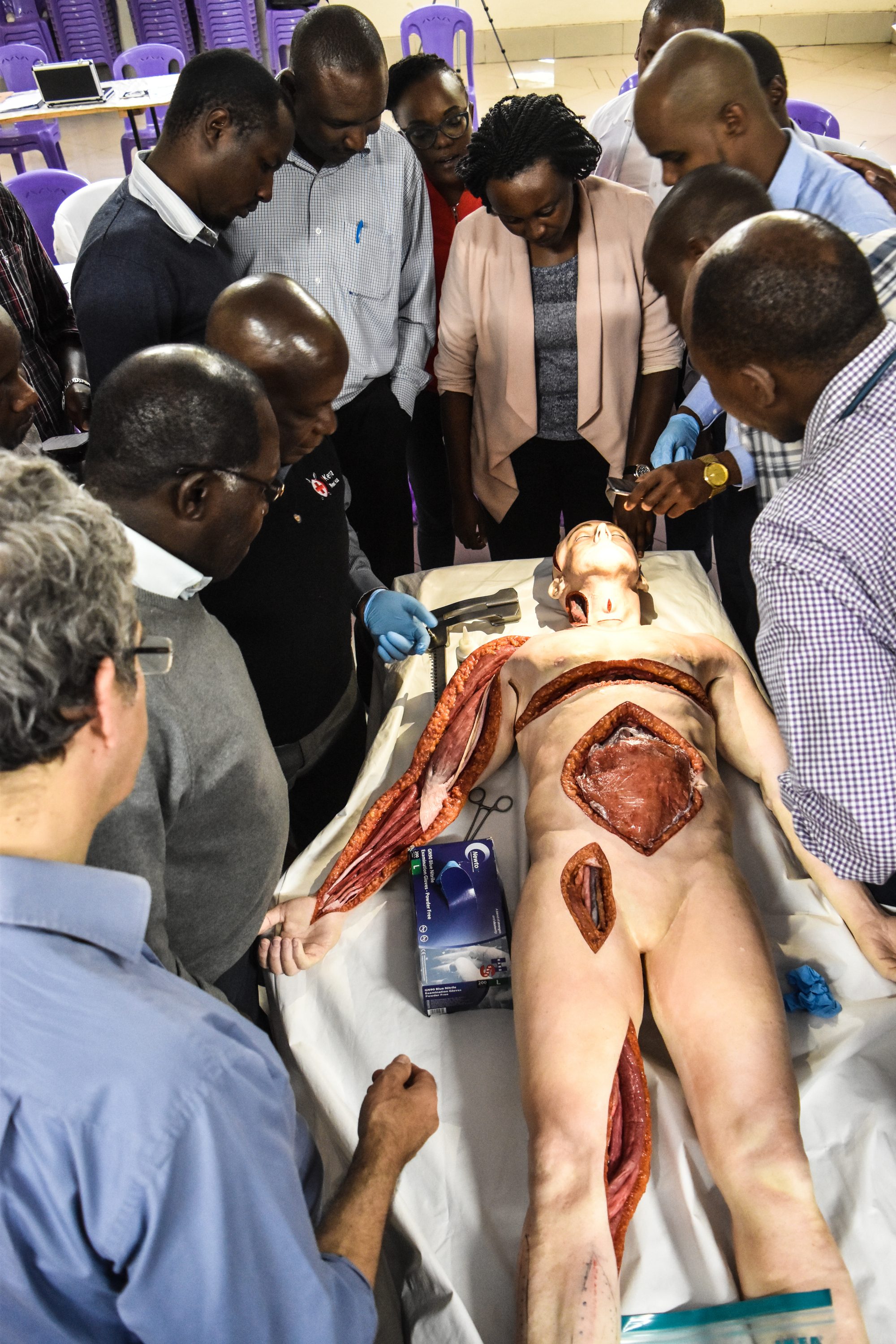
HEST® in Kenya

The Faculty of the David Nott Foundation recently returned from its latest mission to Nakura, Kenya (just a short ride from the capital Nairobi) where it delivered its latest Hostile Environment Surgical Training course.
In partnership COSECSA and Egerton University the Faculty delivered training to 24 surgeons and general practitioners over a 4-day period. During this time, a great range of skills were covered including everything from ballistics examining the effects of low and high-velocity bullets and the stages of a blast injury on the body; vascular surgery and head and neck surgery.
A recent addition to our team (one that comes in the form of a full-body simulator called Heston®) has proven to be one of our most valuable assets. It makes a great addition to the training process, allowing delegates to easily visualise and study further the surgical procedures being taught, with reference to a remarkably accurate human body.
Help us train more surgeons on our HEST® courses by donating www.davidnottfoundation.com/donate

David on the table as Ammar Darwish demonstrates pelvic fracture stabilisation procedures
Surgeon runs the London Marathon

Melanie and her daughter at the London Marathon
“The London Marathon is an iconic event and it was a great privilege to be able to take part with international champions and 42,000 other heroes. I’ve learned a great deal through six months of training and had fantastic support from my family and friends & colleagues at work.
It has been a great experience. Something completely different to my usual life as a colorectal surgeon and mother of three. Raising money for the David Nott Foundation and Bowel Cancer UK has been very important to me. The fundraising has revolved around food – cakes piled up at work with a donation box, fundraising dinners, lastly cake sales at my daughter’s school every day in the week before the marathon.
Read more of Melanie's story here.
STAE course, April 2019


Your support enables us to offer scholarships to surgeons who work in very challenging conditions. It costs £5,000 per student and we cover this entire cost through your generosity. On our most recent course, delivered at the start of April 2019, the training covered how to care for eye injuries from blast wounds, as well as a number of other elements of specialist surgery.
This course was attended by 13 surgeons from countries around the world including Nepal, Syria, Uganda and Chile. The scholars tell us that the way the course is organised is invaluable. “We’re taught the procedure first as a whole group and then get to practice it afterwards in a small team under the supervision team of a surgeon from the Faculty Team,” all of whom are expert surgeons with first-hand experience of working in a conflict zone.
We heard from Vadym who joined us from Ukraine; “This course is way beyond my expectations. It is the best thing that has happened to me in the field of austere environment surgery.”
Paddle Power!

A little over 35 hours is how long it took David Burton and Mattie Morgan to paddle 125 miles from Devizes in Wiltshire to Westminster in central London – a hugely demanding and impressive feat. We are incredibly grateful for their dedication to the Foundation.
You told us what you think!
In response to your comments we will increase the regularity of our newsletter to every 6-8 weeks. We are also aware that people use the website as a primary resource for information - we will continue to make sure it's kept fully up-to-date with all our latest news. We hope you continue to enjoy hearing more about all we do here at the David Nott Foundation.

Kenya HEST® April 2019
The Faculty of the David Nott Foundation recently returned from its latest mission to Nakura, Kenya (just a short ride from the capital Nairobi) where it delivered its latest Hostile Environment Surgical Training course.

Graciously hosted by Egerton University and COESCSA, the Faculty delivered training to 24 surgeons and general practitioners over a 4-day period. During this time, a great range of skills were covered including everything from ballistics examining the effects of low and high-velocity bullets and the stages of a blast injury on the body; vascular surgery and head and neck surgery.


Despite the course being full-on and packed with content, all the delegates were conscientious and showed impressive dedication to learning all they could from the course.
On our HEST® courses it is important to select a curriculum of training we feel will best match the level of ability of delegates in attendance. With the general practitioners being relatively experienced and accomplished surgeons, the level of training was advanced and the quality of interaction all round was excellent.
A recent addition to our team (one that comes in the form of a full-body simulator called Heston®) has proven to be one of our most valuable assets. It makes a great addition to the training process, allowing delegates to easily visualise and study further the surgical procedures being taught, with reference to a perfectly accurate human body.
As ever, we are grateful to our donors for supporting us in our increasingly important work to deliver the best surgical training directly to those who need it most. A recent study in The Lancet showed that nearly 17 million people die prematurely every year from surgically treatable conditions, and that of the 313 million surgical procedures that are carried out each year, only 6% of these take place in the poorest countries worldwide. Furthermore, the study notes that, 5 billion people worldwide do not have access to safe and affordable healthcare and that 143 million additional surgical procedures are needed in lower and middle-income countries in order to save lives and prevent disability.
What this shows then is a lack of, currently, adequate surgical healthcare worldwide, though impacting the poorest nations most. We believe our mission ties in directly with one of the primary needs for the provision of safe surgical care as suggested by the authors of this study: increased numbers of trained surgical providers.
With this in mind, any support you kindly give us goes a long way to tackling this issue that effects so many. Our training serves those on the front-lines. Our training saves lives.


David Nott in conversation with Sarah Montague

On the evening of the 30th April, David was joined in conversation with the BBC’s Sarah Montague at the Saatchi Gallery to discuss his new book, War Doctor. He was sharing stories of his work around the world in war zones and why he and Elly set up the Foundation to share his knowledge and expertise with local doctors working on the ground. Sarah asked him how many lives he thinks he's saved through his own work overseas in war zones and also through our training programme "Possibly in the hundreds of thousands," David replied.
Among the guests was actor and former doctor (of another variety) Peter Capaldi. He noted that the evening was "a humbling and inspiring experience, meeting both David and Elly."

We are delighted to report that, through the generosity of all those who attended the event, enough money was raised to provide equipment to train more than forty surgeons as well as award ten fully-funded scholarships to surgeons currently operating in war zones and disaster areas.

Melanie Feldman runs the London Marathon
Huge congratulations to Melanie Feldman who ran the London Marathon in April. She completed the 26.2 mile race in an impressive 5 hours and 41 minutes. We are very grateful for her hard work raising funds along the way.
Melanie shares her story below:

"The London Marathon is an iconic event and it was a great privilege to be able to take part with international champions and 42,000 other heroes. I’ve learned a great deal through 6 months of training and had fantastic support from my family and friends & colleagues at work. I was part of a Facebook support group for novice marathon runners and that made a huge difference to my preparation with tips and confidence building from a 7000-strong online family. Thanks go to Helen Phillips (The Cheesecake Runner)!
I feel the cold and having spent three hours at Blackheath in the blue start zone I was shivering by the time I got going 45 minutes later. The first half went well; I had been aiming to finish in around 5 hours. Seeing my family at mile 11 was a huge boost. In the second half though I started to get sore and feel sick. The mind remained excited and willing but the legs got stiffer and stiffer. I was desperate for the boost of seeing the family at mile 18 in Canary Wharf... that was the toughest section. From mile 20 I found it was more painful to walk than to carry on my slow jog. By then it looked more like a cyberman shuffle than any sort of running but I was still loving every moment of the day. I crossed over the line in 5:41.
It has been a great experience. Something completely
different to my usual life as a colorectal surgeon and mother of three. Raising
money for The David Nott Foundation and Bowel Cancer UK has been very important
to me. The fundraising has revolved around food - cakes piled up at work with a
donation box, fundraising dinners, lastly cake sales at my daughter’s school
every day in the week before the marathon.
At the end of the day I felt that 26.2 miles is hard - hard training, time away from the family, the weariness if running whilst working and still being part of a family. Half marathons should be enough from now on. But then I entered the ballot once more, so who knows? Maybe there will be another opportunity to experience it once more."

